

To a patient, fascia-focused therapies can seem almost magically simple in their ability to gently relieve pain. But fascia is structurally and neurologically complex. We practitioners need tools that help us to navigate this complexity, to determine how and where fascial restriction is causing problems. The most well-known methods use direct palpation and/or functional tests (motion, gait, muscle weakness, etc.) to find restrictions in fascia, and these are important tools. At Fascia Sense, we are introducing an indirect palpation method based on proprioceptive feedback, which can find primary restrictions quickly and accurately. Called Barrier Depth assessment, this skill is powerful on its own, and can greatly enhance the speed and thoroughness of other assessment methods.
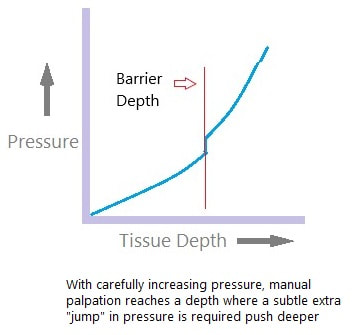
The Barrier Depth (BD) is a particular, measurable quality of surface tissue pliability. BD is found with careful, smoothly increased compression. As illustrated here, it represents an inflection point in a curve where depth of tissue compliance is shown changing with manual pressure. As manual pressure is increased, resistance to compression increases until a point where a sudden "jump" in pressure is required to continue deeper into tissue. After this point, the pressure increase required to go deeper slows down again. The point on the curve right where the additional "jump" of pressure would be required is the Barrier Depth. BD is not obvious with normal palpation techniques but becomes quite easy to detect with proper training and practice.
The Barrier Depth (BD) is a particular, measurable quality of surface tissue pliability. BD is found with careful, smoothly increased compression. As illustrated here, it represents an inflection point in a curve where depth of tissue compliance is shown changing with manual pressure. As manual pressure is increased, resistance to compression increases until a point where a sudden "jump" in pressure is required to continue deeper into tissue. After this point, the pressure increase required to go deeper slows down again. The point on the curve right where the additional "jump" of pressure would be required is the Barrier Depth. BD is not obvious with normal palpation techniques but becomes quite easy to detect with proper training and practice.
With careful palpation, BD reveals restrictions in fascia and other fibrous connective tissue. In short, when engaging with restricted fascia, BD becomes shallower, and during appropriate treatment BD becomes deeper. When treatment is complete, BD becomes "normal", and comparable to the BD of surrounding tissue. To understand this method better, let's take a look at the specifics of how it works:
- Pressure is applied from the surface of the body from two points, while aiming at a third point, somewhere in the fascial system that the practitioner wants to evaluate. The directions of pressure give the best result at an angle close to 90 degrees. As an example, let's say the practitioner's hands are positioned at the posterior and lateral thigh, aiming pressure at approximately 90 degrees, toward deep hamstring musculature.
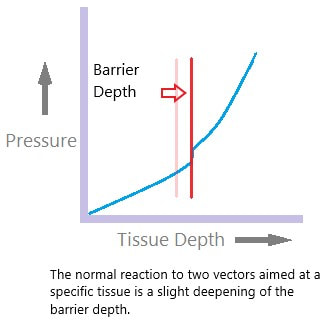
- When the vectors are carefully aimed to intersect at a third point, the normal reaction is a slight deepening of the BD. In other words, the BD of either single hand is less than the BD at both hands when applied simultaneously. This seems to be some sort of whole-body proprioceptive reflex, as the reaction on aiming at a specific site in the body will be the same from any two points of contact (with vectors close to 90 degrees in relationship to each other).
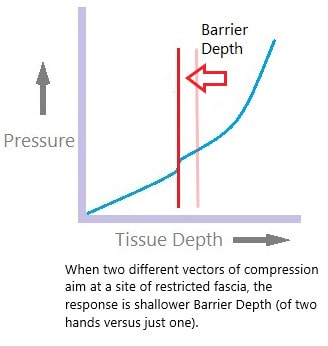
- When the target anatomy has fascial restriction, the opposite happens. The BD with two vectors of compression becomes shallower, at both sites of contact. This is true whether the restriction is intrinsic (stiff fascia) or extrinsic (tight clothing, swelling from injury, interface with implanted hardware, etc.). Again, this seems to be based on a proprioceptive "reflex".
- The degree of decrease in BD seems to correlate with the intensity of "proprioceptive confusion" created by the restriction. This shows up as local or distant effects on muscle tone, isolated muscle strength, range of motion, coordination, etc. In other words, the shallower the BD, the more severe and significant the fascial restriction.
- When treatment is successfully applied, there is typically a shift from shallow BD to deeper than normal BD. In the case of the treatment methods we teach at Fascia Sense Therapeutics, this change in BD is used to guide and monitor the release, making for gentler, faster treatment.
- Finally, completion of treatment is signaled by normalization of BD, with again only slight deepening of BD with two directions of hand pressure, versus just one.