
|
The classic lesion in fascia has been described many ways, including as an "adhesion", or the currently popular term "densification". These terms have more to do with describing what we feel when palpating a fascial restriction, than with what we actually know about the real nature of these restrictions, which is very little. What collective knowledge does say about fascial restriction is that successful treatment comes from direct stimulation, with hands or instruments, to "melt" or "release" the fascia, or to trigger an inflammatory response to promote remodeling. In our treatment system called Residual Strain Therapy (RST), we approach fascial restriction as if it is "residual strain" or stiffening left in the tissue by trauma. The approach uses indirect stimulation, to trigger neurological release of restriction. Learning to release this residual strain can open up a whole new world of ability to help relieve pain, solve difficult cases, and work with an increased confidence in your clinical skills.
What is Residual Strain? Residual strain (RS) is our term for stiffening of tissue in the fascial system, driven by an altered neurological state rather than a physically "densified" change (we know this due to the fact that proper treatment releases a residual strain restriction in as few as two or three seconds). Fascia is basically our organ of proprioception (position sense), and so RS can have a profound impact on proprioceptive feedback, triggering local or referred problems in muscle tone and strength, joint stability, and range of motion. RS can affect a tissue area as small as a carpal ligament or as large as the entire spinal meningeal tube. Areas of RS usually correlate with a past history of intense impact shock, painful injury, repetitive stress, or other high energy input such as sudden stretch or intense vibration (eg. dental drills). 
Getting to the Root of the Problem
After using Barrier Depth palpation to find RS restrictions, the same palpation technique guides the treatment process. Specific points are found on the surface of the body and compressed with a precise direction of pressure, toward the point of restriction. Regardless of how long the restriction has been there, in just a few seconds the RS lesion relaxes to a normal state of tone. The shift typically happens without the client noticing any sensation, although local or distant sensations of heat/cold, tingling or pain may briefly show up. Releasing a particularly strong RS lesion often causes a mild endorphin release, with feelings of relaxation and relief. The change of release is typically permanent, compared to some treatment methods that may get only temporary "release" of fascia. RS is quite common, and we find it as a contributor or cause in a majority of chronic musculo-skeletal pain cases, involved in problems from low back pain and sciatica to shoulder pain and plantar fasciitis. Though less common as a clear-cut cause of more organic types of symptoms, RS sometimes plays a role in problems like vertigo, IBS, or even (rarely) elevated lipids or heart arrhythmias (see sidebar). In our experience, learning to find and treat RS is an essential skill for anyone who wants to offer the most thorough, complete relief options for their suffering patients. In addition, many of our students report that RST treatment makes a big difference for their own health, and for their families. |
Unusual Cases Illustrate the Power of RST
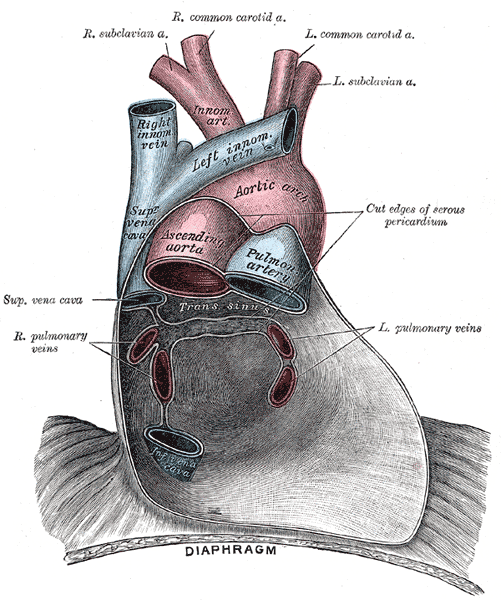
by Dr. Eric Winder The pericardium The fluid-filled organs are dense structures prone to absorbing the energy of an impact shock. Stiffening of the pericardium may be found (from the surface of the body, using Barrier Depth Palpation) after collisions in impact sports, car accidents, or falling backward onto a hard surface. Typically residual strain (RS) of the pericardium has more of an impact on the musculo-skeletal system, contributing to issues like thoracic or lumbar pain. However, over the years I have seen pericardial RS affect heart function. The most dramatic case I have seen of RS affecting the heart was that of a former athlete in impact sports, who had been in two relatively serious car accidents. This patient developed congestive heart failure after an illness, and had very low cardiac efficiency and could fatigue quickly just walking out to check the mail. They could no longer exercise, and were very limited in daily activities. The situation was chronic, and progressively worse over time. Among other areas of RS, the pericardium showed intense RS stiffening. Initial treatment immediately improved spring of the rib cage and inspiratory capacity. After a series of treatments, the patient's energy was returning. Two months later they were doing full workouts at the gym without getting short of breath. The change in physical ability was astounding. In other examples, I have seen treatment of pericardial RS improve arrhythmias, dramatically reduce pain after open heart surgery, and most recently, shorten the regurgitation murmur duration of mitral valve prolapse by 50%. My own benign grade 2 murmur, which started after a car accident, was eliminated by treating pericardial RS, with the change being confirmed by a cardiologist at Harvard University. |
|